

Don't Stuck in the Waiting Room!
Register Online Before You Arrive.
We have up-to-date schedules, contact information, and allow you to make appointments online.
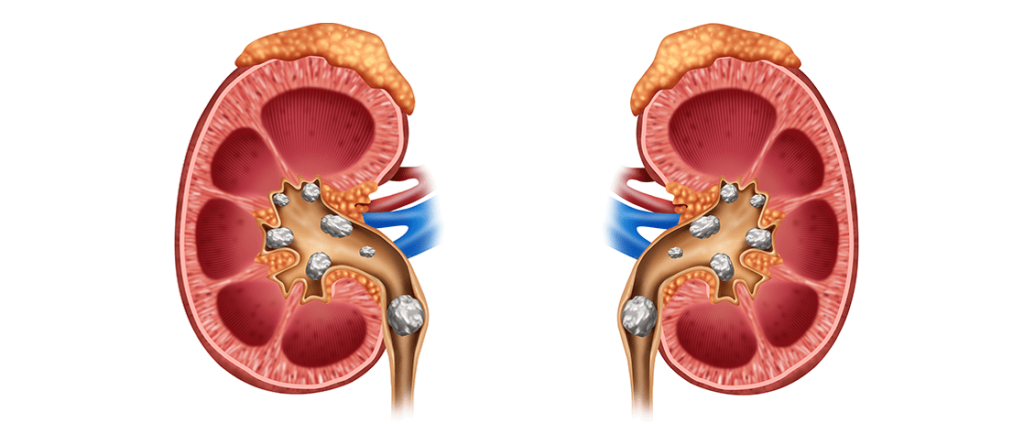
Percutaneous Kidney Surgery in the Treatment of Urinary System Stones (Percutaneous Nephrolithotomy-PCNL)
Percutaneous nephrolithotomy (PCNL) is a safer and minimally invasive approach compared to open surgery for patients with pelvicalyceal system stones. Recent technological advancements have paved the way for the development of endoscopic techniques in treating stones located in the pelvicalyceal system. Over the past decade, indications for PCNL have been more clearly defined, and there has been a general shift toward minimally invasive interventions for treating such stones. Mastery of PCNL techniques is essential for the safe and effective treatment of stone disease. Stones ranging from small renal pelvis stones to staghorn stones can be successfully treated with PCNL.
The percutaneous nephrostomy procedure, similar to the urethra-bladder relationship, creates a channel toward the pelvicalyceal system and serves as the foundation for every percutaneous intervention in the upper urinary system.
Initially, percutaneous nephrostomy was used solely for urinary diversion, but today it is necessary for initiating more complex procedures such as stone removal. In the early 1980s, the introduction of extracorporeal shock wave lithotripsy (ESWL) temporarily reduced the indications for stone-targeted percutaneous interventions. However, once the limitations of lithotripsy became apparent, PCNL regained its rightful role in stone treatment.
Compared to open surgery, percutaneous renal interventions are significantly less morbid and cause less discomfort to the patient. Moreover, obese patients benefit greatly from this procedure. Pearle and colleagues found that the stone-free rates in obese patients (body mass index >30) undergoing percutaneous nephrolithotomy were comparable to those in the unselected patient group. The complication and transfusion rates, as well as the length of hospital stays, were also similar. However, in this group of patients, modifications to the standard technique and instrumentation may sometimes be necessary for percutaneous nephrostolithotomy.
Many urologists have limited experience in accessing the pelvicalyceal unit, and thus some centers may require the assistance of interventional radiologists. However, to remain at the forefront of endoscopic urology in the era of minimally invasive interventions, all urologists must master the technique of percutaneous kidney intervention.
Basic Anatomy
Urologists must accurately understand the anatomy of the kidney and its relationship with surrounding structures. Understanding the stereotactic form dynamically is essential in preventing complications during percutaneous surgery.
The kidneys are located in the retroperitoneum between the T12 and L2-L3 levels. Since they are situated on the psoas muscle on the posterior abdominal wall, the long axes of the kidneys are parallel to the oblique course of the psoas. They almost always show some rotation, with the upper poles closer to each other than the lower poles. The kidneys form a 30° angle with the posterior frontal plane of the body, and the right kidney is situated 2-3 cm lower than the left. The diaphragmatic movement during respiration causes the kidneys to move downward and upward during inspiration and expiration, respectively.
Typically, there are upper, middle, and lower major calyx groups, but a variety of variations can be seen. The upper and lower major calyces are whole and extend at different angles toward the pole regions. Middle calyces are arranged as anterior and posterior sections. Sampaio reported that in 96% of cases, the upper pole drains into the midline calyx infundibulum, based on a study evaluating 140 pelvicalyceal systems using three-dimensional polyester resin casts. The middle section is drained by double calyces arranged in two rows (anterior and posterior) in 96% of cases and the lower pole in 58% of cases. The study’s results suggest that reaching a pole region drained by a single infundibulum is easier than reaching a region drained by double calyces.
The main renal artery divides into anterior and posterior branches. The anterior branch further divides into four anterior segmental arteries supplying the anterior and pole regions. The posterior segmental artery supplies the remaining posterior portion of the kidney. In more than 50% of kidneys, the posterior segmental artery is localized in the upper half and middle of the posterior side of the kidney and can be damaged by a more medial needle entry into the upper calyx.
After passing through the renal sinus, the segmental arteries divide into interlobar arteries, which become arcuate arteries at the corticomedullary junction. Interlobular arteries are right-angle branches of the arcuate arteries. The Brödel line describes the avascular plane between the anterior and posterior regions. By following a posterolateral transparenchymal path, the needle crosses the Brödel line, avoiding damage to major blood vessels. Directing the needle transparechymally towards the posterior calyx reduces the likelihood of significant bleeding.
In terms of patient satisfaction, the main goal in the treatment of stone disease is how much stone burden can be managed and the cost. For these reasons, alternative treatment methods should be explained to the patient, and the most appropriate treatment method should be recommended.
DO YOU NEED HELP?
Request a Callback Today!
We will usually contact you within 24 hours of your request.